-
Credits
- Section Writer: Dr. Om J Lakhani
- Section Editor: Dr. Om J Lakhani
- Last update: 02-Sep-2023
-
Q. How common are aggressive pituitary tumors (APT) ?
- 15% of pituitary adenoma
-
Q. How common is pituitary carcinoma?
- very rare - 0.1-0.4% of Pituitary adenoma
-
Q. What is the definition of pituitary carcinoma ?
- Distant metastasis or metastasis beyond the craniospinal axis
-
Q. At what age are they seen ?
- generally in older people - in 5th decade and beyond
-
Q. Which type of adenomas are more likely to be aggressive ?
- Corticotroph adenoma
- Lactotroph adenoma
-
Q. What is an important point in history that correlates with aggressive pituitary tumor (APT)?
- Headache
- Presence of headache in pituitary tumor is because of
- Highly proliferative tumors
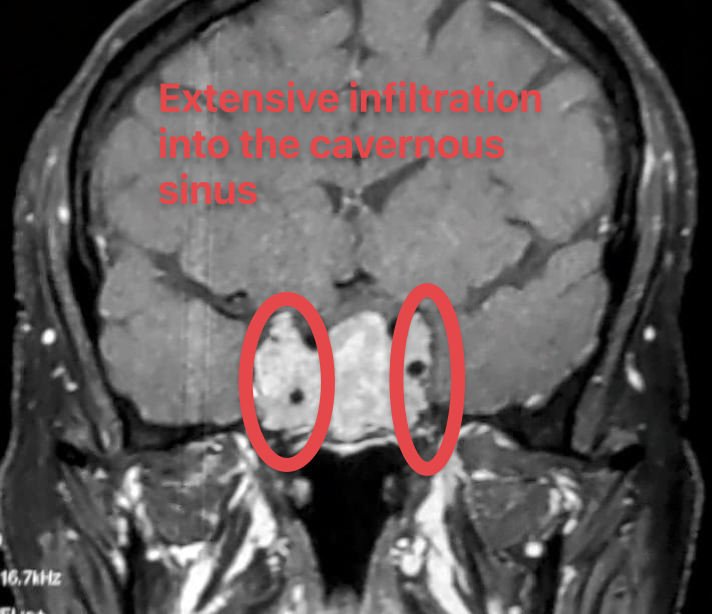
- Cavernous sinus invasion
- presence of somatotroph adenomas
-
Q. Are they more common in MEN1 syndrome ?
- Yes
-
Q. Is there any specific definition or diagnostic criteria for APT ?
- No
- There is a general definition given by ESE which is
- "PAs that demonstrate radiological invasiveness and an unusually rapid tumor growth rate, or clinically relevant tumor growth despite optimal standard treatments in the form of surgery, radiotherapy, and conventional medical therapies"
-
Q. What percentage growth can be considered rapid ?
- More than 20% increase of maximum diameter of the pituitary adenoma over 12 months is considered rapid growth
-
Q. Clinically based on response to treatment, what is considered APT ?
- Progression or recurrence of tumor after radiotherapy is considered to be important marker of APT
-
Q. Based on immunohistochemistry, how do you define APT ?
- Ki-67 index >3%
- elevated mitotic index
- more than 2 mitosis per 10 HPF
- extensive p53 immunostaining >10
-
Q. What Ki-67 index is suggestive of Pituitary carcinoma ?
- More than 10% - Pituitary carcinoma
-
Pearl:
- Ki-67 >3%- Aggresive pituitary tumor
- Ki-67 >10%- Pituitary carcinoma
-
Q. Is invasiveness same as aggressiveness ?
- No
- An invasive tumor need not be aggressive and may still respond to treatment (eg: Invasive prolactinoma)
- If tumor is invasive and aggressive- it has worst prognosis
-
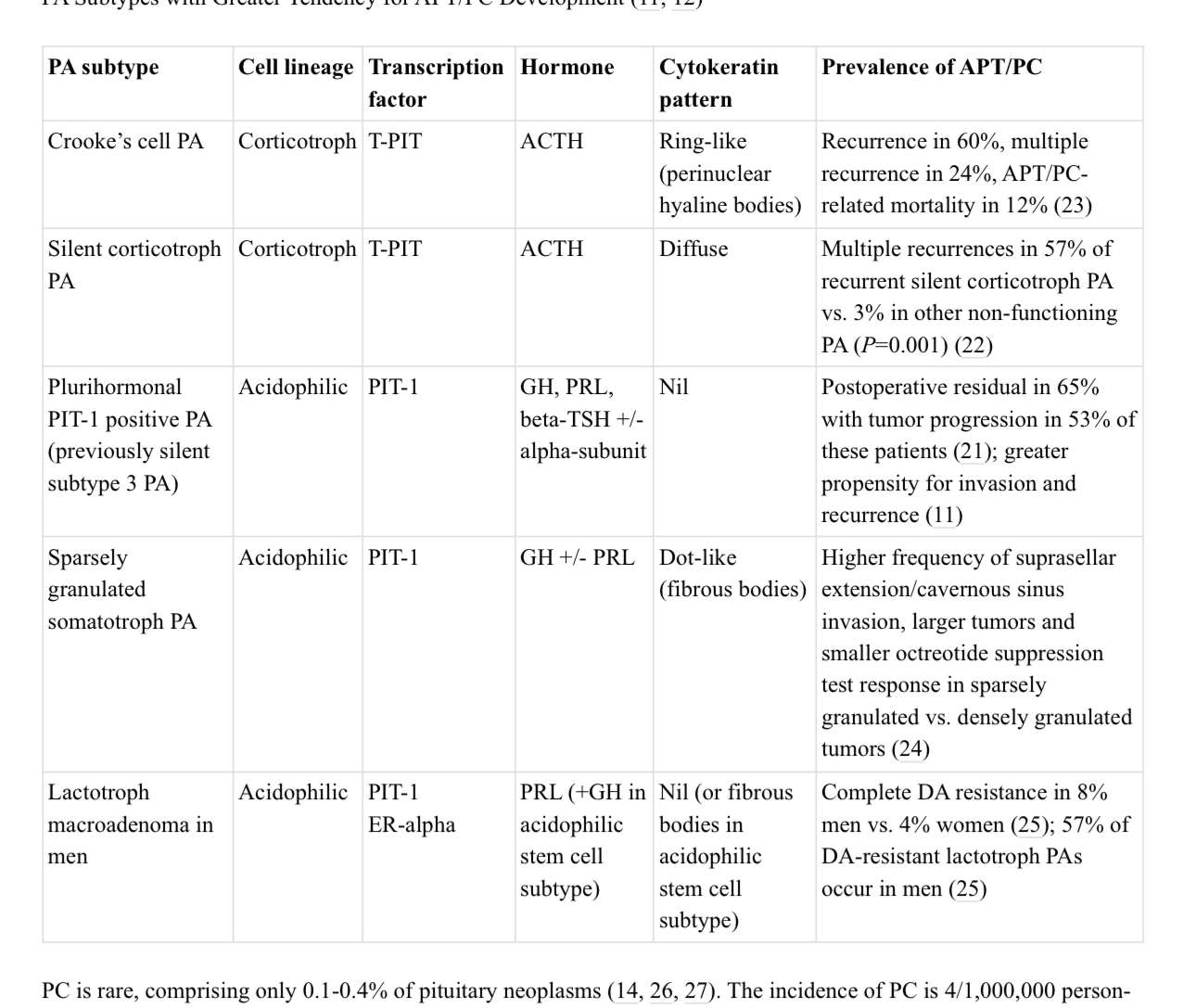
Q. Which type of pituitary adenomas are generally more aggressive ?
-
- Pituitary adenoma in children
-
- Silent corticotroph adenoma
-
- Crooke's cell pituitary adenom2
-
- Plurihormonal PIT-1 positive adenoma
-
- Sparsely granulated somatroph adenoma
-
- Lactotroph macroadenoma in men
-
-
Q. Can a microadenoma be aggressive ?
- Generally rare for that to happen
-
Q. Which symptoms are more suspicious of aggressive pituitary adenoma ?
- Cranial nerve palsies
- Obstructive hydrocephalus
-
Q. Which "named syndrome" related to pituitary is a form of aggressive pituitary adenoma ?
- Nelson's syndrome is a form of aggressive pituitary adenoma
-
Q. It is a generally dictum that pituitary adenoma do not cause Diabetes insipidus. Which Pituitary adenoma can cause DI ?
- Metastasis to posterior pituitary from primary pituitary malignancy can cause DI
- However, in such cases other primary causes like breast and lung cancer also need to be ruled out- DI due to these are much more common
-
Q. Which are the common site for metastasis for pituitary malignancy ?
- Brain
- Spine
- Liver ==> Commonest site for Corticotroph adenoma
- Cervical lymph nodes
- Bone ==> commonest site for Lactotroph adneoma
-
Q. Should genetic testing be done in patients have aggressive pituitary adenoma ?
- Yes
- Germline genetic testing should be offered to patients having aggressive pituitary adenoma
-
Q. When should adjuvant radiotherapy be considered post surgery ?
- If there is clinically relevant invasive tumor remanent with pathological markers of aggressive tumor (Ki-67, Mitotic count and p53) - then in that case adjuvant radiotherapy may be considered
-
Q. What are the biochemical markers of Acromegaly remission used in clinical studies ?
- IGF-1 - Normal range
- GH - <2.5 ug/l
-
Q. Which is the only pituitary directed therarpy approved for Cushing's disease ?
- Pasireotide
- However the experience of the same in aggressive corticotroph adenoma is limited
-
Q. What is the definition of complete resistance of prolactinoma to dopamine agonist ?
- Failure to normalize prolactin
- Failure of >50% reduction in size of adenoma
- When doses of carbergoline >3.5 mg/week have been used
-
Q. Can cabergoline be increased to >3.5mg ?
- Yes
- The maximum tolerated dose must be used
- Some case reports have used upto 11 mg/week with tumors responding to that dose
-
Q. What kind of transcription factor is expressed by gonadotrope tumors ?
- SF-1
-
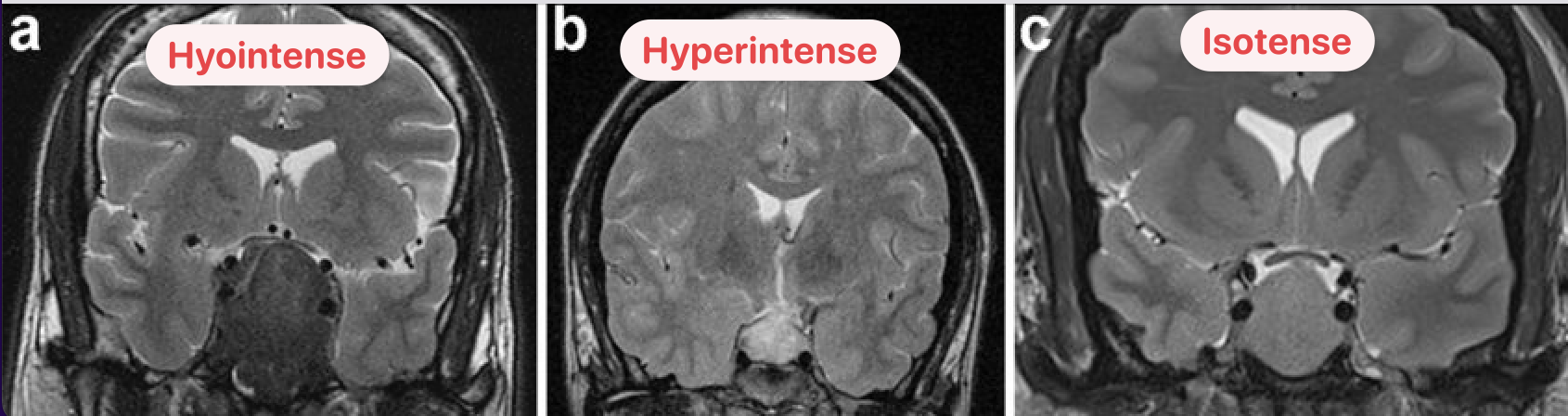
Q. What is the importance of T2 weighted images in Acromegaly ?
- T2 hyperintensity compared to normal pituitary adenoma or normal gray matter in a somatrotroph adenoma is associated with sparsely granulated tumor which is associated with more aggressive behavior
-
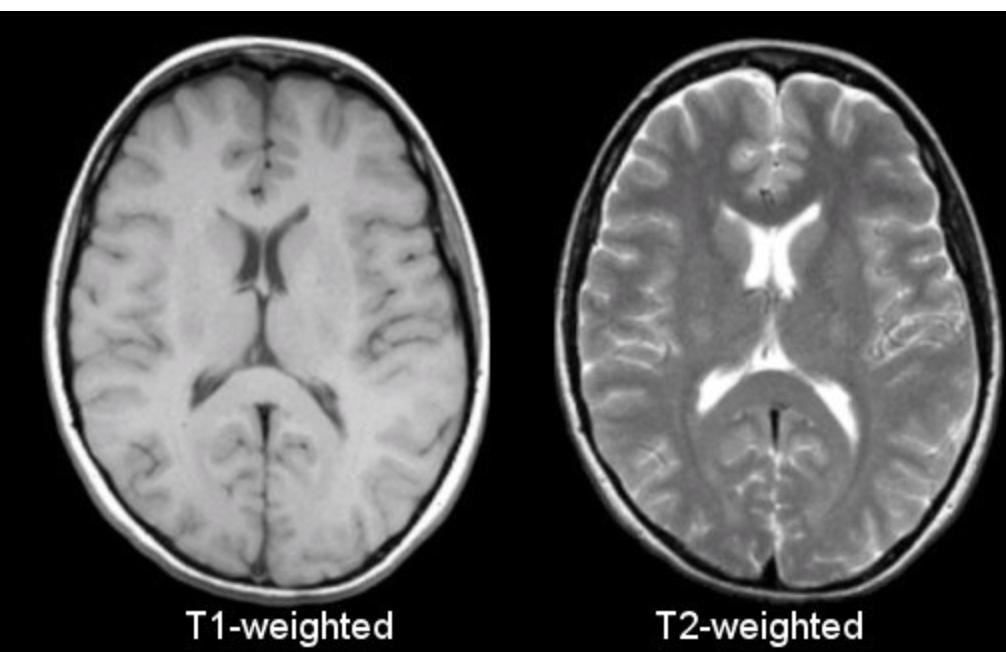
Q. How to identify T2 sequences ?
- Remember the CSF appears white in a T2 sequence
-
Q. What is the criteria based on MRI to consider a Pituitary adenoma as invasive ?
- Knosp grade 3 and 4 correlates with radiological invasion
-
Q. What is the Knosp's criteria ?
- The Knosp criteria is a classification system for pituitary tumors based on their invasiveness into surrounding structures, specifically the cavernous sinus. The criteria is based on the tumor's size, location, and degree of invasion, and ranges from grade 0 (no invasion) to grade 4 (complete invasion). This classification is used to help guide treatment decisions for pituitary tumors.
-
Q. How is the size of Pituitary adenoma best determined on serial scans ?
- The largest diameter is to be considered on 1 Dimension
- This correlates with size on 3D
-
Q. What is the ideal classification system to use for Cavernous sinus invasion ?
- Knosp classification of cavernous sinus invasion

- Grade 0 - adenoma does not extend the medial carotid line.
- Grade 1 - adenoma extends the medial line, but doesn't reach the median line, so-called “intercarotid” line.
- Grade 2 - tumor extends beyond the median line, but doesn't extend beyond or tangent to the lateral line.
- Grade 3
- 3A - the tumor extends to the lateral line superiorly (over ICA)
- 3B - the tumor extends to the lateral line inferiorly (under ICA)
- Grade 4 - The tumor totally wraps around the intracavernous carotid artery
-
Q. On a Knosp classification, when do you say for certain that cavernous sinus is invaded ?
- You say this when the tumor cross the outer border of the carotid artery present in the cavernous sinus
- This is grade 3 or greater as per the Knosp classification
-
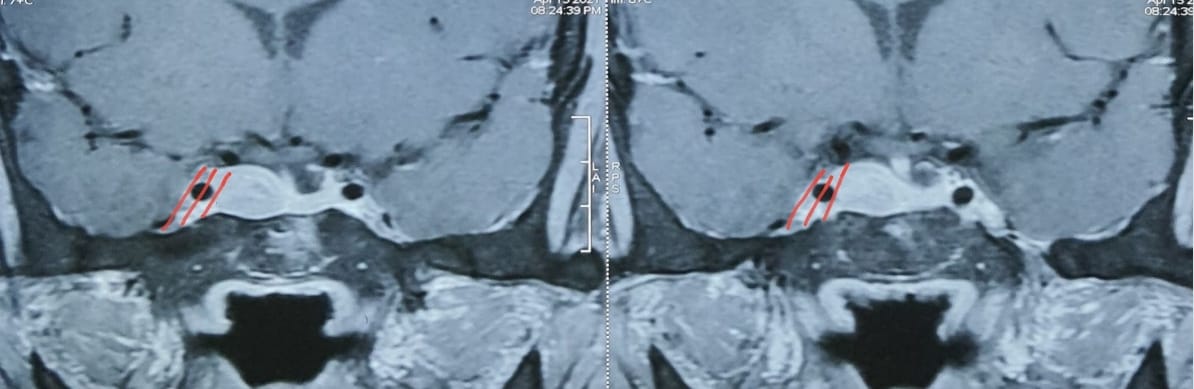
- Patient with recurrent pituitary adenoma with Knosp classification of Grade 3C
- Patient with recurrent pituitary adenoma with Knosp classification of Grade 3C
-
Q. What is MRI volumetric analysis
- MRI volumetric analysis is a technique used to measure the volume of different structures in the brain or other organs using MRI imaging. It involves processing MRI images to create a 3D reconstruction of the region of interest and then using specialized software to segment the image into different structures or regions. By measuring the volume of these structures, researchers or clinicians can quantify changes in size over time or compare volumes between different individuals or groups
-
Q. Does PET scan have any role of Pituitary imaging ?
- Gallium DOTATE may be useful for assessing the extent of spread in Pituitary carcinoma
-
Q. What receptor determines the response to medical therapy in case of somatotroph adenoma ?
- SSTR2 expression
- more the expression- better the outcome
-
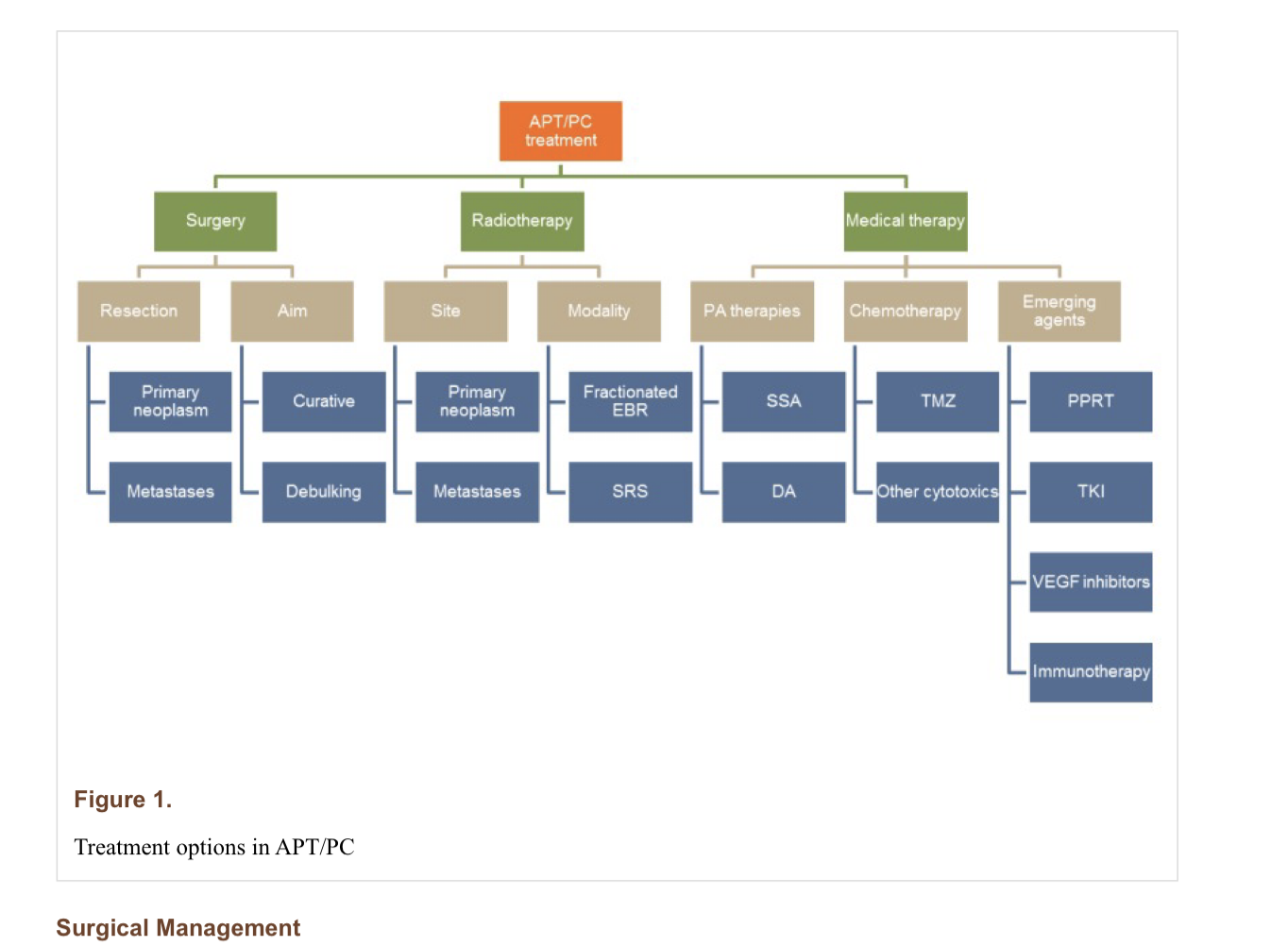
Q. Give the outline for management in case of Aggressive pituitary tumor (Atypical pituitary tumor) and Pituitary carcinoma ?
-
Q. If radiotherapy is considered , what should be done- fractionated radiotherapy or Stereotactic radiosurgery ?
- The choice of radiotherapy is not dependent on aggressiveness of tumor but rather dependent on the safety features- eg- closeness to optic chiasma etc
-
Q. What is the role of PRRT in patients with Aggressive pituitary tumor (Atypical pituitary tumor) and Pituitary carcinoma ?
- PRRT has limited role in patients with aggressive pituitary adenoma
- A recent review of 20 PRRT-treated APT/PC cases reported in the literature found limited success, with partial responses in 3/20 and stable disease in 3/20.
- Patients on Temozolomide tend to have almost no response
-
Q. True or false, Aggressive pituitary tumor (Atypical pituitary tumor) and Pituitary carcinoma respond poorly to standard medical therapy for functional pituitary tumor ?
- True
- However, dose escalation is often helpful
-
Q. What does of Carbergoline have been used in patients with Lactotroph adenoma which are aggressive ?
- Doses as high as 11 mg/week have been used
-
Q. What are the medical options for Lactortroph adenoma (Prolactinoma) not responding to cabergoline ?
- Temozolomide can be given
- Some Lactoroph adenoma express SSTR5 and may respond to Pasireotide though this has been described only in selected cases
-
Q. Is Pasireotide more effective than first generation somatostatin analgoues ?
- Yes
- Pasireotide is a more effective second generation somatostatin analogue than first generation somatostatin analogues in treating acromegaly and Cushing's disease, and is more effective in normalizing IGF-I and GH levels and reducing tumour volume in acromegaly, and is more effective in normalizing UFC levels in Cushing's disease.
- Pasireotide is also more effective in reducing tumour size in thyrotroph tumours.
- Prolactinoma do not respond to first generation agent but may respond to Pasireotide
-
Q. What is the difference between Pasireotide and standard first generation somatostain analogues in terms of their action of somatostain receptors ?
- Pasireotide binds to multiple somatostatin receptors, including SSTR2A and SSTR5, while standard first generation somatostatin analogues only bind to SSTR2A.
-
Q. Which is a chemotherapeutic drug used for aggressive pituitary tumor ?
- Temozolomide has been used in various case series for aggressive pituitary tumor
- It is found to be reasoably effective in several case series
- However, there are no large RCT for the use of this drug
-
Q. What is the dosing schedule for Temozolomide ?
- 150 to 200 mg/m2 once daily for 5 days of each 28-day treatment cycle until disease progression for up to a maximum of 12 cycles
-
Q. What do the ESE guidelines say about Temozolomide ?
- They recommend the use of the drug for 3 cycles
- If radiological progression is seen-they recommend stopping the drug
-
Q. Can Temozolomide be combined with other drugs ?
- Yes
- Several combinations have been tried including Capecitabine, bevacizumab, thalidomide etc
-
Q. How is Temozolomide available in India ?
- It is available as Capsule Temoside 100 mg or 250 mg dose. Available as a bottle/strip with 5 capsule.
-
Q. What are the common side effects of Temozolomide ?
-
- Fatigue is the most common side effect
-
- LFT monitoring must be done
-
- Nausea and vomiting may occur- so anti-emetic may be prescribed during the fist cycle
-
- Hematological monitoring is required- Myelosupression may occur
-
-
Q. Can Temozolomide be combined with Radiotherapy ?
- Yes.
- This is called the "Stupp protocol"
- Initially the drug is given in dose of 75 mg/m2/day along with 6 weeks of EBRT
- The logic is that the drug improves the response to radiotherapy
- This is followed by the standard regimen of 150-200mg/m2- for 5 days every 28 days for 6 months
-
Q. How long is Temozolomide given in patients with aggressive pituitary adenoma ?
- Treatment should be continued for at least 3-6 months, and should be stopped if there is progressive disease or serious adverse events occur.
- Typical duration is 12 months
- In ESE survey treatment has been given for often for mean of 9 month to upto 36 month in some cases
-
Q. What happens after stopping Temozolomide therapy ?
- After stopping Temozolomide, there is often a period of sustained remission with a median time to progression of 12 months.
- Patients receiving more than 12 months of TMZ achieved a median relapse-free survival of 57 months compared with 18 months in those receiving less than 12 cycles.
-
Q. What are the determinants of the response to Temozolomide ?
- The determinants of the response to Temozolomide include the MGMT status, the presence of mutations in the mTOR pathway, the expression of ErbB receptors, and the type of pituitary tumor or carcinoma
-
Q. What is the relationship between MGMT expression and response to Temozolomide ?
- Low MGMT expression is associated with a positive response to Temozolomide, while high MGMT expression is associated with a lack of response.
-
Q. How is the MGMT expression determined ?
- MGMT expression is determined by immunohistochemistry (IHC) markers of pituitary tissue by experienced neuropathologist
-
Q. What are the treatment options for atypical pituitary tumor beyond Temozolomide (TMZ) ?
- Treatment options for atypical pituitary tumors beyond Temozolomide (TMZ) include everolimus therapy, lapatinib therapy, EGFR/ErbB2-targeting lapatinib therapy, mTOR pathway STK11(F298L) mutation, and ErbB receptor expression targeting.
-
Q. Can a second trial of TMZ be given to patients who have relapse ?
- Yes, a second cycle of TMZ may be given to patients with atypical pituitary tumor, but it is rarely reported to be successful in such cases.
-
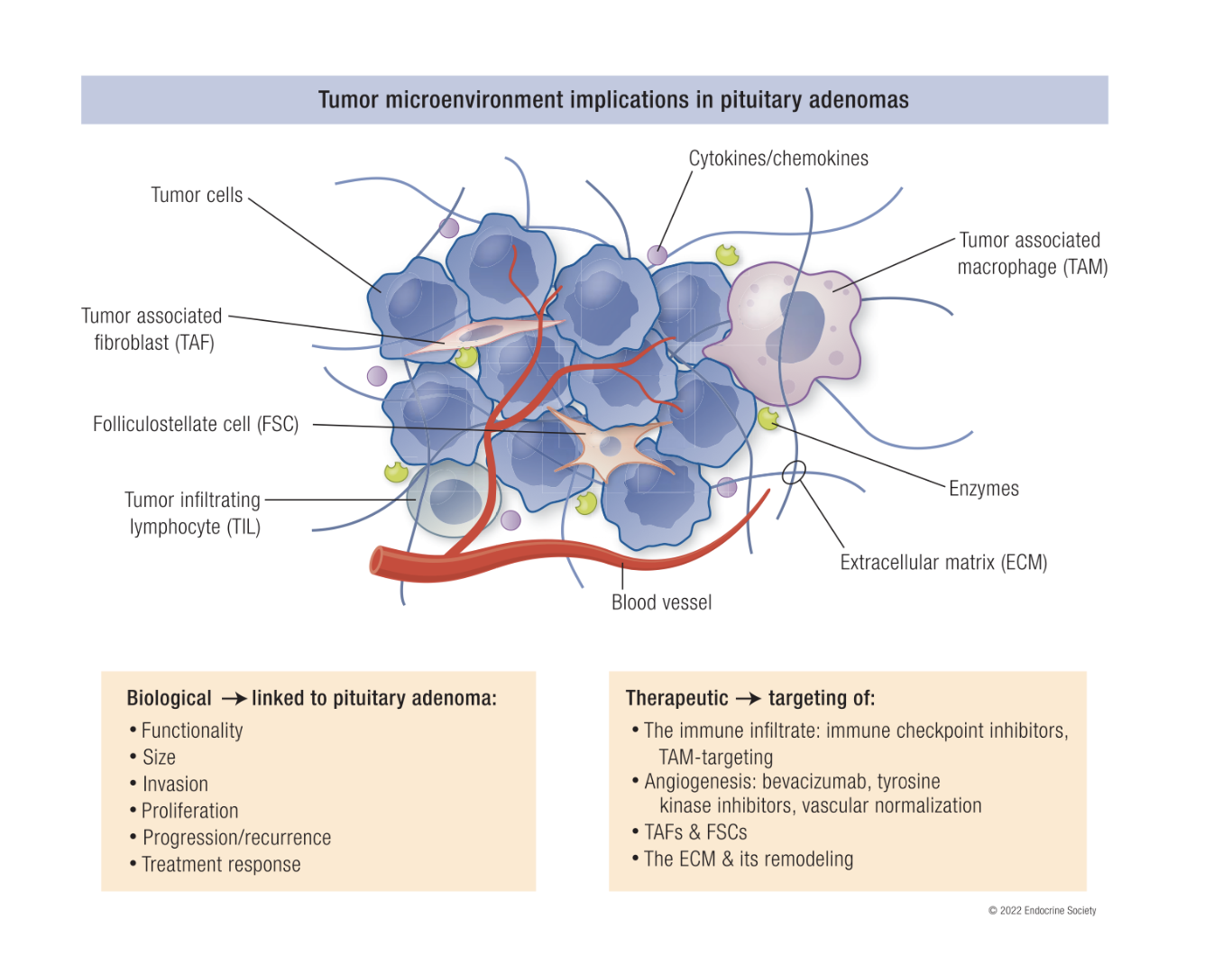
Q. Can you give a picture of the Tumor microenvironment and it's implications on pituitary adenoma treatment ?
-
Q. Which are the most important and abundant cells in the tumors which are associated with tumor related issues ?
- Tumor associated macrophages- are the most important cells
- They are associated with size, invasion and proliferation - mainly invasion of pituitary adenoma
-
Q. Which drugs are showing promise in treatment of aggressive pituitary adenomas and pituitary carcinomas ?
-
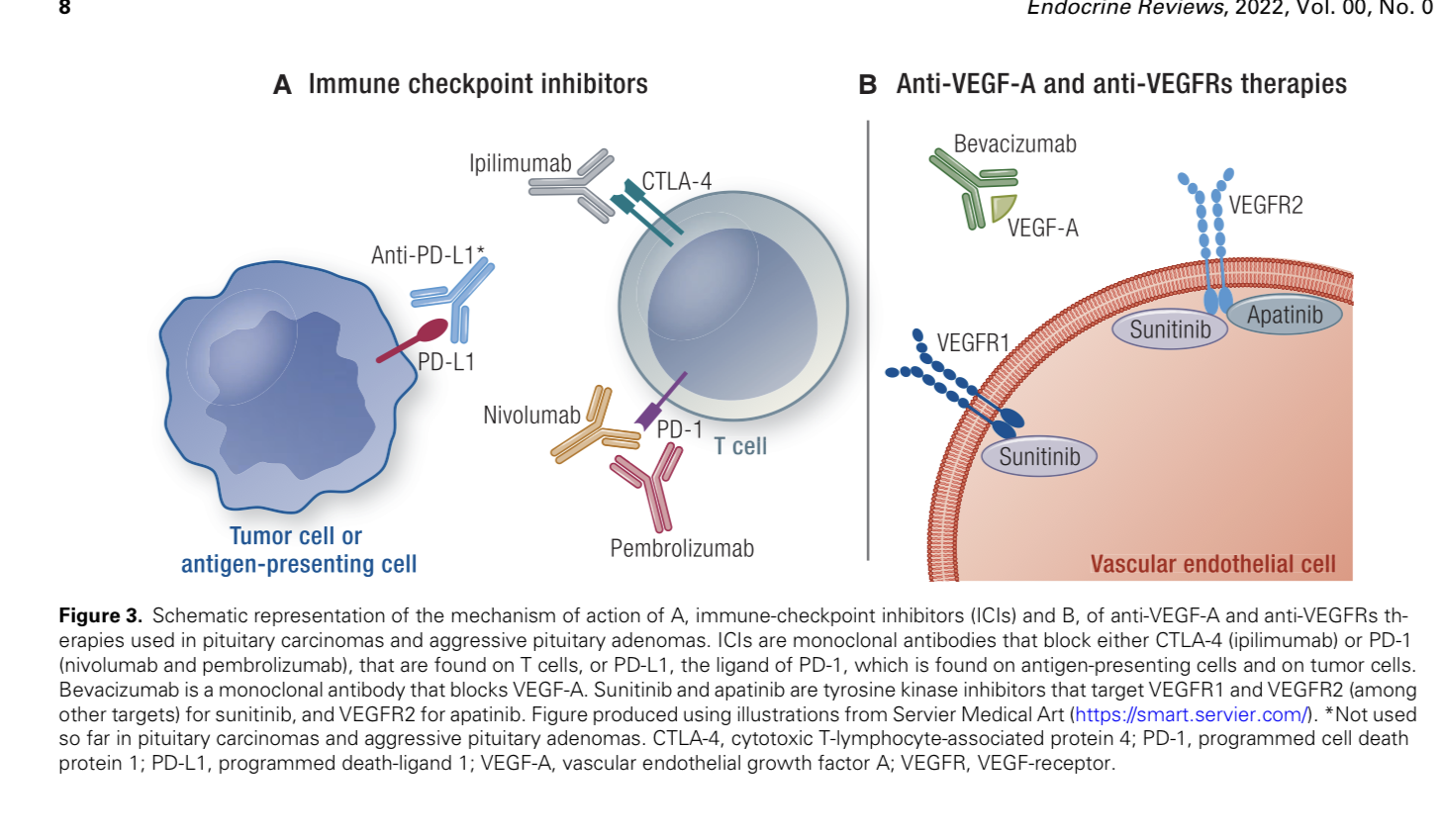
Q. Tell me more about the role of immunotherapy in APT ?
- Immunotherapy may play a role in the management of APT by reducing immune tolerance and increasing T-cell concentration.
- It has been suggested that anti-CTLA4/PD1 therapy may be successful in treating corticotroph PC
-
Q. Which are the various immune check point inhibitors ?
- Antibodies against CTL4
- Ipilimumab
- Tremelimumab
- Antibodies against PD-1
- Pembrolizumab (Keytruda) ·
- Nivolumab (Opdivo) ·
- Cemiplimab (Libtayo)
- Antibodies against PD-L1
- durvalumab
- atezolizumab
- avelumab
- Antibodies against CTL4
-
Q. What is this therapy with Immune checkpoint inhibitors called ?
- Tumor microenvironment based therapy
-
Q. What is the overall prognosis of patients with APT ?
- The overall prognosis of patients with APT is difficult to determine due to the variable course of the disease and the lack of data on long-term outcomes. Generally, APT is associated with a worse prognosis than PA, with a higher rate of recurrence and a greater risk of metastasis. However, some APTs may respond well to standard treatments and never exhibit aggressiveness.
-
Q. What is the importance of the somatic expression of ATRX gene in APT ?
- ATRX is important in APT because it is a gene that is associated with aggressive pituitary tumors and pituitary carcinomas.
- Mutations in the ATRX gene can lead to the development of these tumors, and understanding the role of ATRX in APT can help researchers develop better treatments for these tumors.
- Somatic variants of ATRX as seen in 1/5th of APT
- This may be exploited as an IHC marker in the future
-
Q. What in the new radiotracer that has been found to be used in pituitary tissue tracing ?
- C11 Methionine is a specific tracer of pituitary tissue
- It is more specific than FDG-PET
- It may play an important role in future
-
Q. What is an alternative terminology suggested for Pituitary adenoma ?
- It is suggested that pituitary adenomas should be called "Pituitary neuroendocrine tumors" instead